Video 4
Tips and Tricks in Laparoscopic Surgery – Port Placement
Introduction
This is my 4th video in the series Tips and Tricks in Laparoscopic Surgery. In this Video I am going to look at different ways of Port placements. Whenever I teach laparoscopic suturing, the first question I ask my students is “what is your preferred port placement”. There is no point learning how to suture with one port placement and go back to perform surgery with a different port placement. So deciding on which is your preferred port placement is important before embarking on laparoscopic surgery. In this video I will discuss the different types of port placements and their advantages and disadvantages. In the discussion that follows, I am assuming that the surgeon is right handed and stand on the left side of the patient when performing laparoscopic surgery.
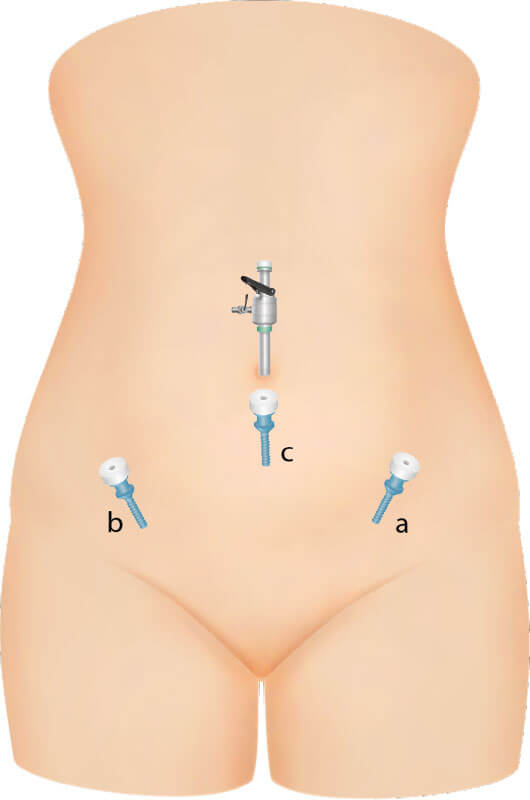
Besides the camera port, 2 other ports are placed to perform the surgery. The port placement is usually on either side of the abdomen as shown in the diagram below. The surgeon has his right hand at port b and the left hand at port a.
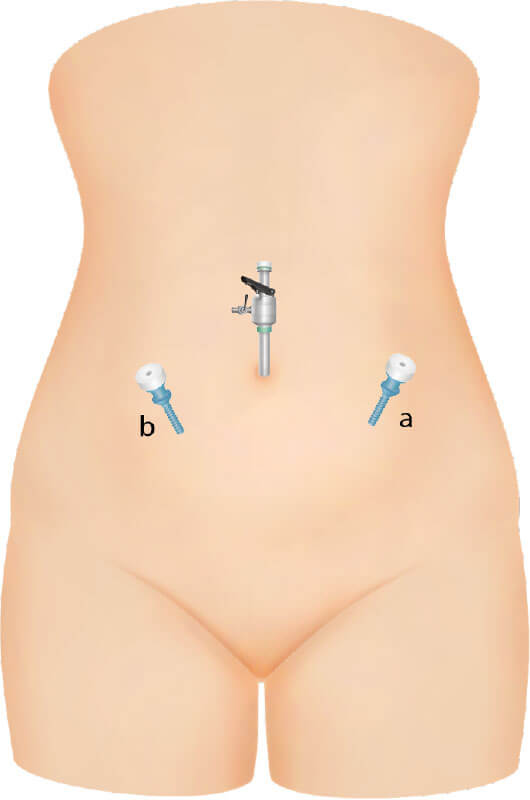
This strategy is done under several circumstances:
- In an easy case, another port will not make much of a difference.
- The assistant is not competent and is not able to assist with another instrument and so will only hold the camera for the surgeon.
When this strategy is used, usually the surgeon will use in his dominant right hand to hold at point b an instrument that has many functions such as coagulation and cutting properties. Examples of such instruments are Enseal, Ligasure and Caiman.
The only advantage I can see of this technique is that the patient may perceive that cosmetically 3 scars are better than 4 especially when these 2 ports are placed very low down along the bikini line.
The disadvantage is that it may be difficult to perform advanced cases because of the lack of another instrument to assist in the surgery. The time taken to perform the surgery may also be longer.
There are basically 3 ways of placing the ports in a 4 port strategy
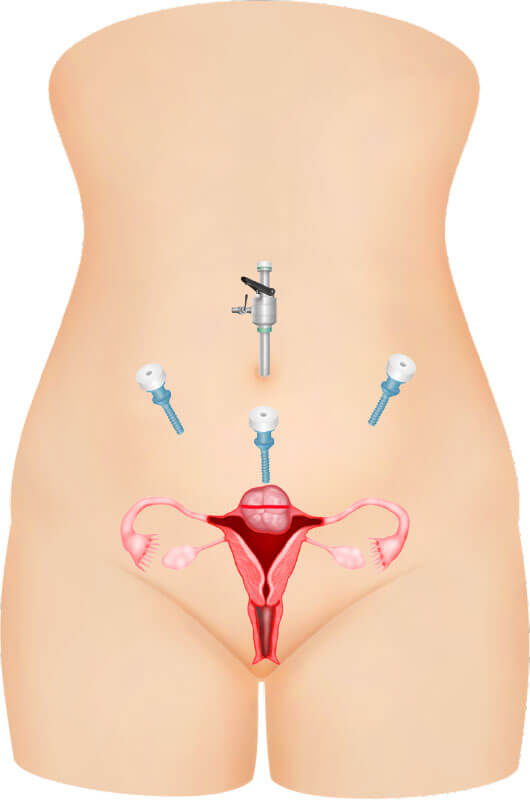
- Contralateral ports
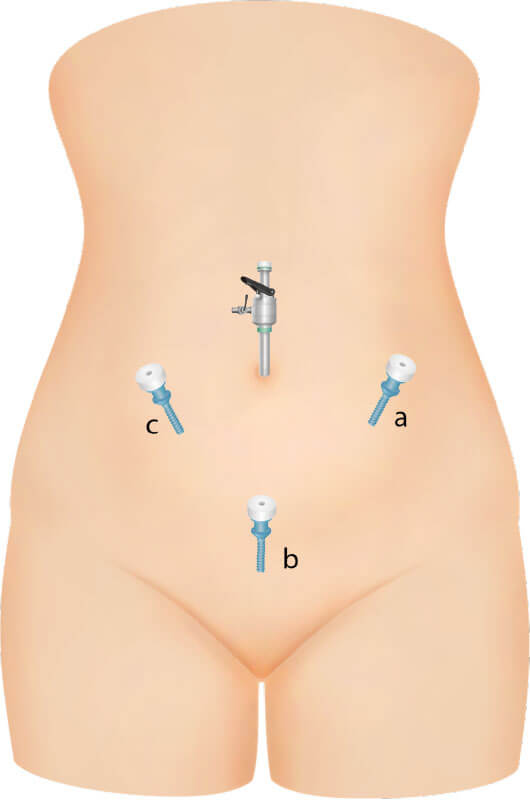
- Suprapubic ports
- Ipsilateral ports
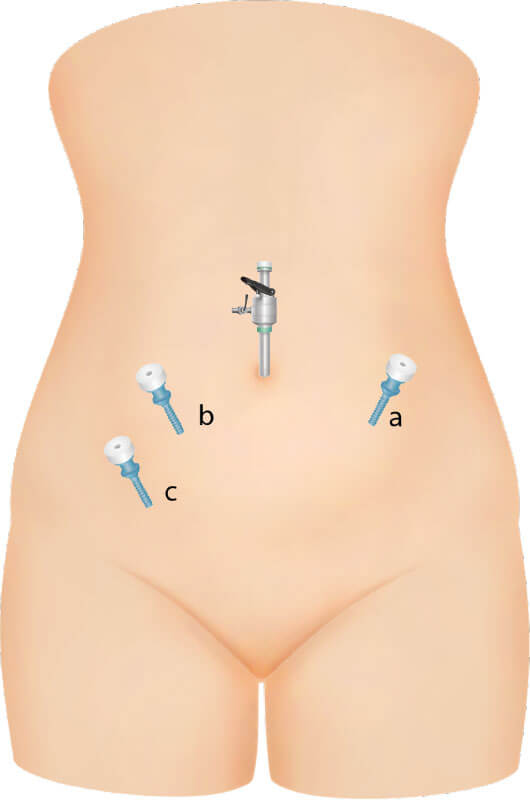
A variation of this I saw when operating with the late Dr. Rakesh Sinha where he placed the assistants port in the lower abdomen on the right side at “c”.
In that situation he had 2 assistants, the assistant holding the camera standing on the right side and another assistant standing on the left side holding the instrument at “c”. This technique is not common.
Advantage of Contralateral ports
- It is easy to tie knots because the instruments are at right angles to each other
- The surgeon can dissect both sides easily, the right hand can dissect the left side of the pelvis and the left hand can dissect the right side of the pelvis
Disadvantage of contralateral ports
- It can be tiring as the arms are separated and adducted
- The right arm may block the assistant holding the camera
- You need to be tall to do this technique. Shorter surgeon will find it difficult to hold the instrument on the right side.
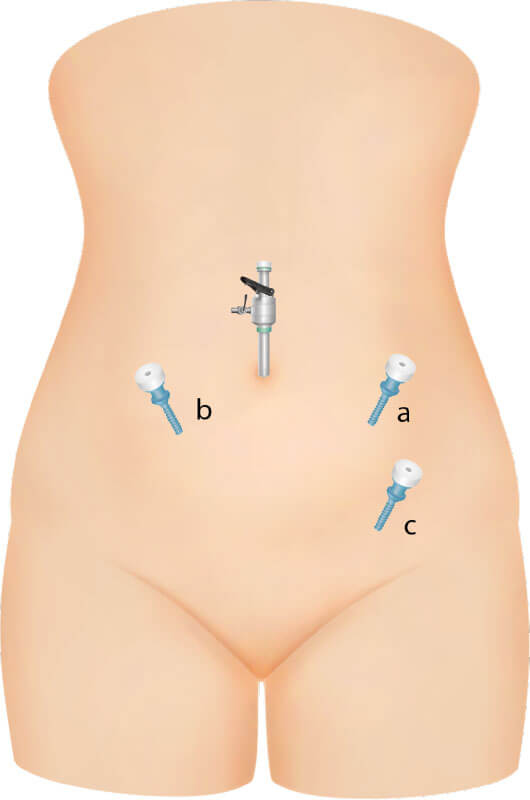
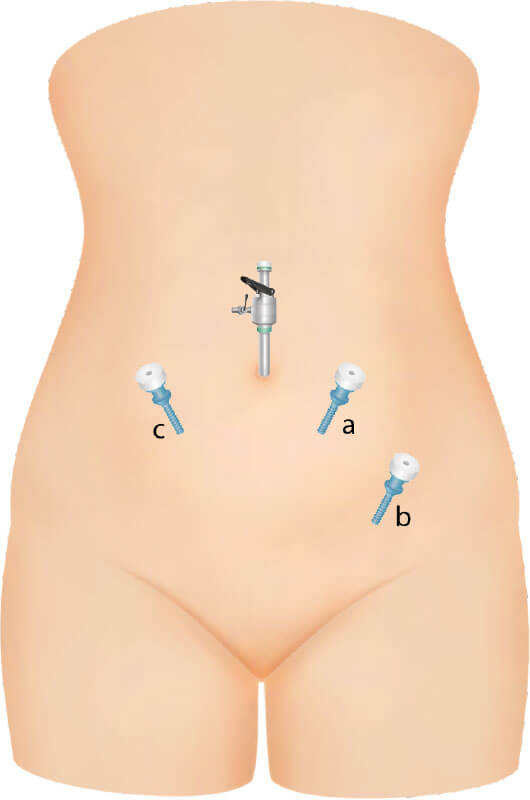
In this technique, one of the surgeon’s port will be on the left side and the second will be in the midline somewhere between the symphisis pubis and the camera port.
In his technique, Prof Wattiez places the left port (a) very low down, just above the ASIS (anterior superior iliac spine). His suprapubic port (c) is higher than the left lateral port. In this way the port placement will make him operate in a very comfortable position. Both his arms are down and not abducted.
The disadvantage is that you need to be good with your left hand suturing because it is impossible to suture with your right hand from the left port (a)which is placed so low down.

Prof Ando places his left port “a” higher up sometimes almost at the level of the umbilicus. The midline port is usually somewhere between the pubis and the camera port. In this technique the left hand of the surgeon will need to be closer to the patient’s abdomen and may be slightly uncomfortable. The right hand at port b is mostly abducted and high up. The advantage of this technique is that one can switch your right hand from the suprapubic port ‘b” to the left hand port “a” especially when performing suturing during laparoscopic myomectomy. Suturing a transverse or oblique incision from the suprapubic port can be awkward.
Prof Nam of Korea operates slightly differently. His left sided port “a” is high up at the level of the umbilicus. He uses his right hand to hold instruments here and his suprapubic port ‘b” is very low down sometimes just above the symphisis pubis. He uses his left hand to hold instruments here. He does most of his surgeries in this position. The advantage of this technique is that the left hand at the suprapubic port ‘b” can be used to dissect on either side of the pelvis. His right hand at port “a” can be used to dissect and suture as well. The disadvantage is that since the suprapubic port being so low down you cannot use your right hand at this port to perform surgery. It can only be used to retract and assist in the surgery.
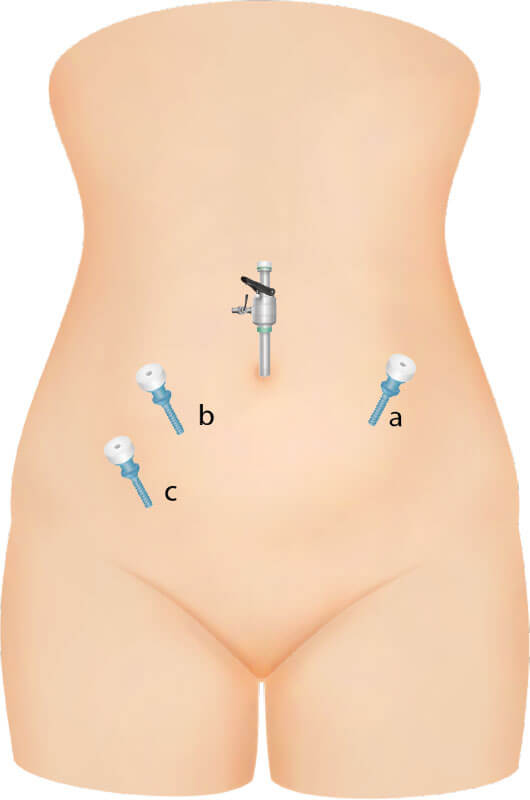
Here the surgeon’s 2 ports are on the left side of the abdomen. The advantage of this port placement is that the surgeon’s arms are low down comfortably when performing surgery. There will be less lethargy when operating. Then disadvantage is that during suturing the instruments are almost parallel to each other so tying knots can be difficult. The other disadvantage is that ¬
There are some variations to placement of the ipsilateral ports
a. Both the left ports are in the same line
This is the classical ipsilateral port placement.
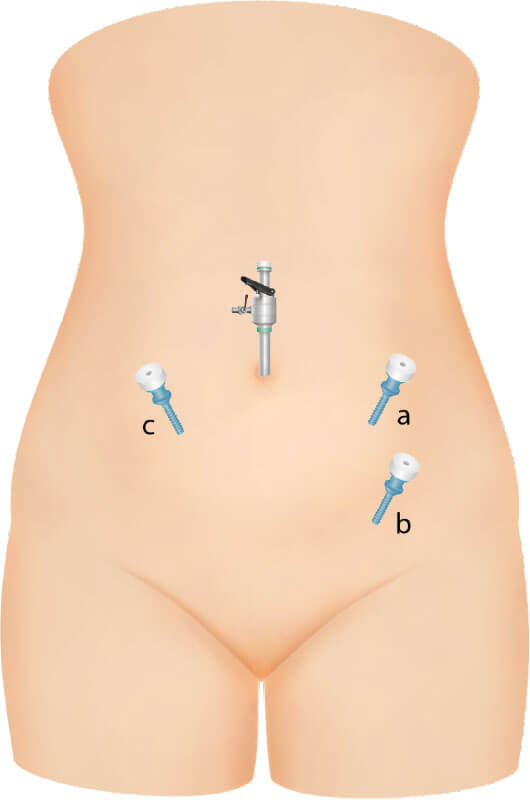
Since the ports are on the same line, the instruments may clash as you point to the pelvis. .
b. Modified ipsilateral – Dipak Limbachiya’s technique
I have described this port placement in my earlier video. Here a line is drawn between the left lower port ‘b” and the camera port. The left port ‘a” is placed half way between these ports. The advantage of this technique is that the right hand is more forward compared to the left hand and so the right arm is in a more comfortable position. There will be less clashing of the instruments in the pelvis. It is also easier to access the left side of the pelvis. The disadvantage is that
c. Dr. Charles Koh and Dr. Shailesh Puntambekar’s technique
Dr Charles Koh and Dr Shailesh who are both right handed but they operate from the right side of the patient. Here the right hand port “c” is low down just above the ASIS and the left hand port “b” is higher up about 4 finger breath below and on the right of the camera port. Dr Charles Koh vows that this is the best position for the right handed surgeon especially for suturing. Unfortunately for me I could not master this technique because my assistants who are nurses could not learn to assist me from the left side.
Conclusion
There is no one perfect port placement. You have to decide which port placement is good for you. Always remember that you can move your right hand to the assistant’s port to perform surgery if you find your port placement awkward in certain situations. For example when doing laparoscopic sacrocolpopexy where a lot of suturing is required, I suture from the right port when it is not possible to do suturing from the suprapubic or ipsilateral ports. Another tip is that, if you find the ports not conducive for a particular operation, don’t hesitate to place more ports. Another small 5mm scar will not do much harm to the patient.
For more than 20 years I was using Dr. Ando’s technique of port placement. I was having frequent right arm and right sided neck pain. Since switching to the ipsilateral port of “Dr. Dipak”, I could still do most of the dissections which I was doing with the suprapubic port but with less injury to my arm and neck. I believe that standing and holding the instruments comfortably is important especially when performing long surgeries.
Selva
Sevellaraja Supermniam
4/5/2020
www.melakafertility.com