Tubal ligation (also known as having one’s “tubes tied”) is a surgical procedure for sterilization, in which a woman’s fallopian tubes are permanently closed. Tubal ligation is considered a permanent method of birth control. It is usually performed via the laparoscopic route (see chapter 22). Some patients find themselves wanting to conceive again later in life. Reasons include divorce and a new marriage, loss of a child, or simply the realization that they would like a larger family. Such women who have previously undergone tubal ligation and want to have another baby, may request for a reversal of the tubal ligation.
There are 2 ways in which a woman who had previously undergone a tubal ligation could conceive again. The first is by a surgery to reverse the tubal ligation and the second is by Invitro-Fertilization (IVF). It is important to understand the advantages and disadvantages of each technique before deciding, which technique will be suitable for the couple.
Comparison of the advantages and disadvantages of laparoscopic tubal reversal and IVF
Comparison | Tubal ligation Reversal | IVF |
|---|---|---|
Advantages | Advantages One procedure More Natural Able to treat other gynaecological diseases at the same time | Can work with low sperm count Faster and non surgical |
Disadvantages | Surgery General anaesthesia Risk of ectopic pregnancy Surgical discomfort 5% tubes cannot be repaired If unsuccessful, then IVF Need for future contraception | Ultrasound guided
Sedation anaesthesia Risk of multiple pregnancies Ovarian Hyperstimulation 5% -10% of cycles cancelled If unsuccessful, then try again Tubes still “tied” |
The advantages of tubal ligation reversal are that after a successful surgery to “open up” the tubes, the couple can attempt to conceive every month. If she successfully conceives, then she can have as many pregnancies as she desires. The disadvantage is that, if only 1 pregnancy is desired, she will need to have future contraception. There is also a 5% incidence of ectopic tubal pregnancy after the tubal ligation reversal.
Traditionally, tubal reversal is performed using a large incision (laparotomy) and microscopes or other image-enhancing devices. The recovery time could be several weeks. However, now this surgery can be performed laparoscopically.
The most important factor that determines the success of tubal reversal surgery is the technique of tubal ligation that had been performed. During tubal ligation, a part of the tube is destroyed (see chapter 22). The lesser the damage the better the chances of pregnancy after tubal reversal. Generally, a patient who has undergone tubal ligation using clips (figure 22.1) will have the best success rate because the amount of tubal destruction will only be 4 mm. If the fimbrial ends of the tubes have been removed (fimbriectomy), the success of tubal reversal will be the lowest. Tubal ligation by coagulation or by suturing, and cutting of the tubes will depend on the length of the normal tubes left behind for reconstruction. The shorter the amount of tube that is left behind after the tubal ligation, the poorer the success of pregnancy after the reconstruction.
Preoperative assessment
A review of the operative notes on the technique used for the tubal ligation performed previously could be useful. If the technique of tubal ligation performed involved the loss of most of the tubes, then IVF may be a better option to achieve a pregnancy. Often, information on the previous tubal ligation may not be available. In such an instance, it may be necessary for the patient to undergo a diagnostic laparoscopy first, to see whether the tubes are amenable for reconstruction. If they are not suitable for repair, than the tubal reversal is abandoned and the patient can proceed with IVF. However if the tubes look sufficiently good for repair, tubal reversal surgery can proceed as planned.
The surgery
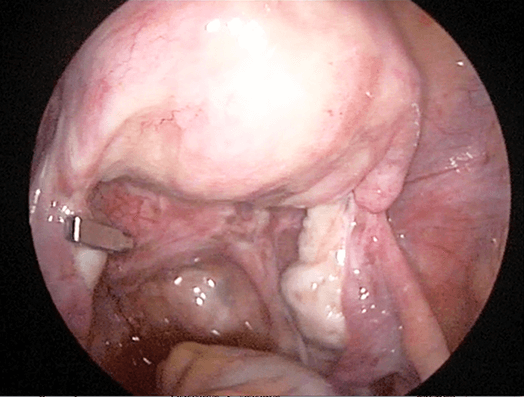
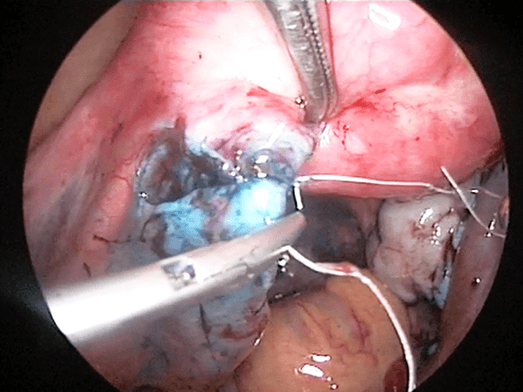
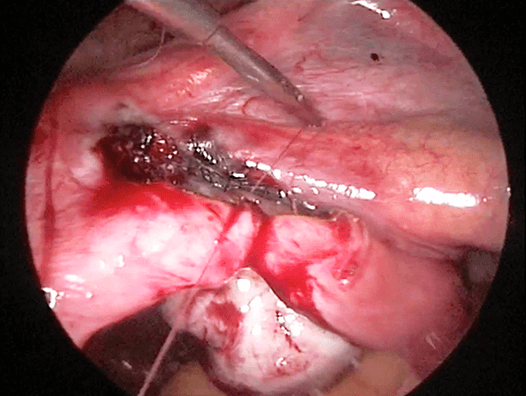
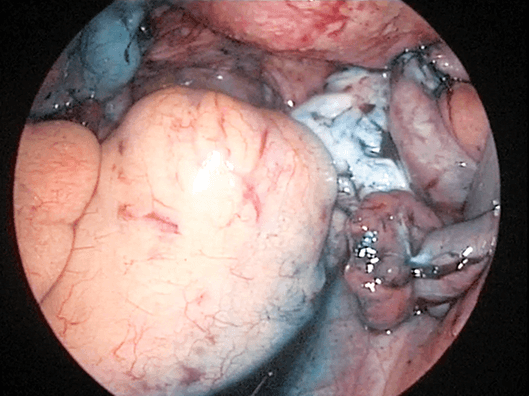
Laparoscopy is performed in the usual manner (see Chapter 15). After placing the laparoscope to visualize the uterus, tubes and ovaries, 3 secondary trocars are placed for the introduction of the microsurgical instruments. These are finer instruments compared to the instruments used in normal laparoscopy. The tubal block is removed and the two segments of the tubes are prepared to be connected. The part of the tube that remains attached to the uterus is called the proximal end; and the other part with the fimbrial end is called the distal part of the tube. A blue dye is injected via the cervix to see if the proximal part is patent. In order to determine whether the distal part of the tube is patent, a probe is placed at the fimbrial end and a blue dyed fluid is injected. If the dye comes out of the other end, then the distal end of the tube is patent. Another method is to pass a fine tube through the cervix and into the fallopian tube from the proximal end into the distal end and out of the fimbrae. This will also assist in the alignment of both parts of the tubes for connection. The 2 ends of the tubes are then sutured together using fine sutures. Suturing of the 2 parts together requires advanced surgical techniques. The process is repeated on the other tube. Once the connection of both tubes is completed, a blue dye is injected through the cervix and if the dye is seen flowing out of both the fimbrial ends, the surgery is considered a success.

Case 28.1
Spontaneous pregnancy after reversal of tubal ligation
Madam CYL was a 32-year-old lady who consulted me in June 2009. She had had 2 children and a tubal ligation using Filshie’s clips in 2005. She remarried and wanted a reversal of the tubal ligation. She underwent a tubal reversal in July 2009 (watch video 27.1). She subsequently conceived spontaneously and delivered a healthy baby girl in December 2010.
Learning point
This lady underwent a tubal ligation at 28 years of age. This may be considered too early an age to undergo a tubal ligation. In this patient the reversal of tubal ligation was successful for several reasons. The first reason is that she was young and so did not have any problems with ovulation. Secondly, because Filshie’s clip was used, the amount of tissue damaged during the tubal ligation was small and so the surgery to reverse the tubal ligation was successful.
Pregnancy
Patients should wait for three months prior to attempting pregnancy in order to give the tubes a chance to heal completely. Trying to conceive before that could result in an increased risk of ectopic tubal pregnancy
Summary
Reversal of tubal ligation can be performed laparoscopically. The success of this surgery will depend on the technique of the tubal reversal. The longer the length of tubes left behind after the tubal ligation, the better
is the success of tubal ligation reversal. The best chance of success occurs when the tubal ligation was done using clips.