“ A specialist is one who has made all the possible mistakes that can be made in a very narrow field” – Niel Bohr
Complications occur in any form of surgery, may it be laparotomy or laparoscopy. The more experienced a surgeon is, the less likely that a complication may occur. It is important to know about all the possible complications that could occur before embarking on a surgery.
Complications can occur during the 2 different steps of laparoscopic surgery.
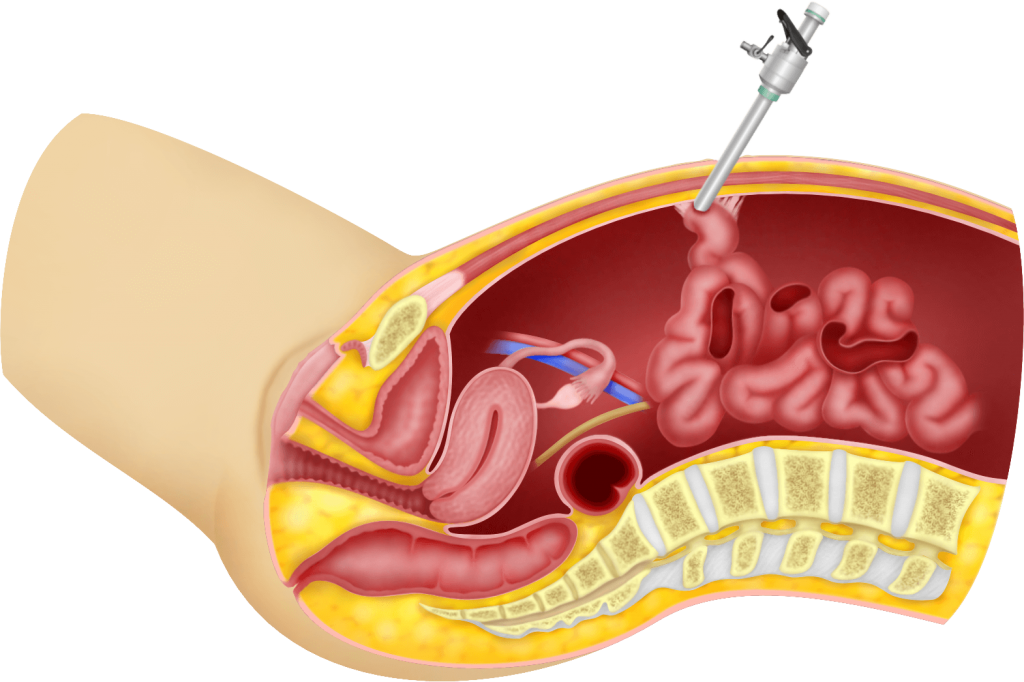
1) During the first step of passing carbon dioxide into the abdominal cavity (creating the pneumoperitoneum) and while inserting the trocars and the laparoscope.
2) During the surgical procedure itself.
1) During the first step of passing carbon dioxide into the abdominal cavity (creating the pneumoperitoneum) and insertion of the trocars and the laparoscope
a) Placement of the first trocar.
Complications can occur in the placement of the first trocar. There are many ways of placing the first trocar. The first technique is by using a Veress needle to introduce carbon dioxide into the abdomen (insufflation) and blindly placing the first trocar through the umbilicus. If there are adhesions of the intestines to the abdomen especially at umbilical site, injury to the intestines may occur. If this injury is noticed, the injured intestines can easily be repaired either laparoscopically or via a laparotomy.
There are several strategies to reduce the incidence of this complication.
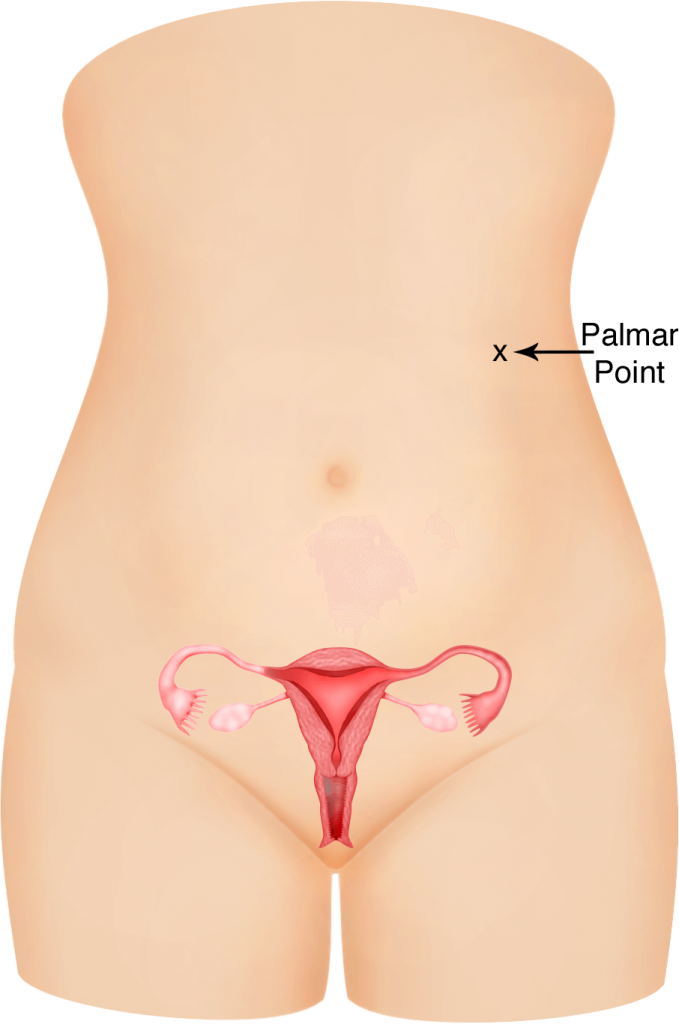
i) Verres at the Palmar point
If adhesions are suspected, as in patients with previous midline laparotomy surgery, then a Veress needle can be placed at the Palmar point (a point just below the left costal margin at the midclavicular line). Carbon dioxide insufflation can then be done from this position. A 5 mm trocar can be placed at this site to visualise the abdomen and pelvis and to look for any adhesions before proceeding to place all the other trocars. The incidence of adhesions at the Palmar point is very low and so the risk of organ injury while starting laparoscopy from this site, is safe. However, the disadvantage is that the trocar placed at this site is an extra incision which is difficult to use during the surgery. The patient may end up with more than 4 wounds in the abdomen.
ii) Open Laparoscopy
Open laparoscopy is a technique whereby an incision is made in the umbilicus so the rectus sheath (g) and peritoneum is opened under direct vision. Once the abdominal cavity is penetrated, a trocar is placed into the abdomen and insufflation is done.
As this is not a blind procedure, any bowel adherent to the umbilicus will be seen through this incision, and if bowel injury does occur, repair can be done immediately. Studies show that this method does not reduce the incidence of bowel injury but if it does occur, it will be easily detected. The disadvantage is that the incision made in the umbilicus is usually larger and there may be leakage of gas from the large incision, making surgery sometimes difficult. In order to avoid the leakage of carbon dioxide, a sleeve called the “Hasson sleeve” can be added to the trocar to plug the leak. A purse string suture can also be placed around the trocar to tighten the tisssues around the trocar.
iii) Optical Trocar
Nowadays, trocars are hollow and their sleeves come with transparent tips. This type of trocar allows a laparoscope to be placed in it while it is inserted into the abdomen. With the laparoscope in its sleeve, the trocar is rotated and it can be seen penetrating the subcutaneous layer, rectus sheath and finally the peritoneum. This can be done before or after insufflation. This technique removes the worry of blind insertion of the trocar. This again will not prevent bowel injury but if injury does occur it will be detected and repaired immediately. The disadvantage of this method is that while optical trocars are disposable, they are quite expensive.

iv) Ternamian trocar
A ternamian trocar is a special trocar which has an extra “screw thread” on it. After insufflating the abdomen with carbon dioxide, this trocar can be “screwed” into the abdomen with a laparoscope placed in it. Just like the optical trocar, this trocar can be seen penetrating the subcutaneous layer, rectus sheath and finally the peritoneum. Again, this will not prevent bowel injury, but if injury does occur it can be detected and repaired.

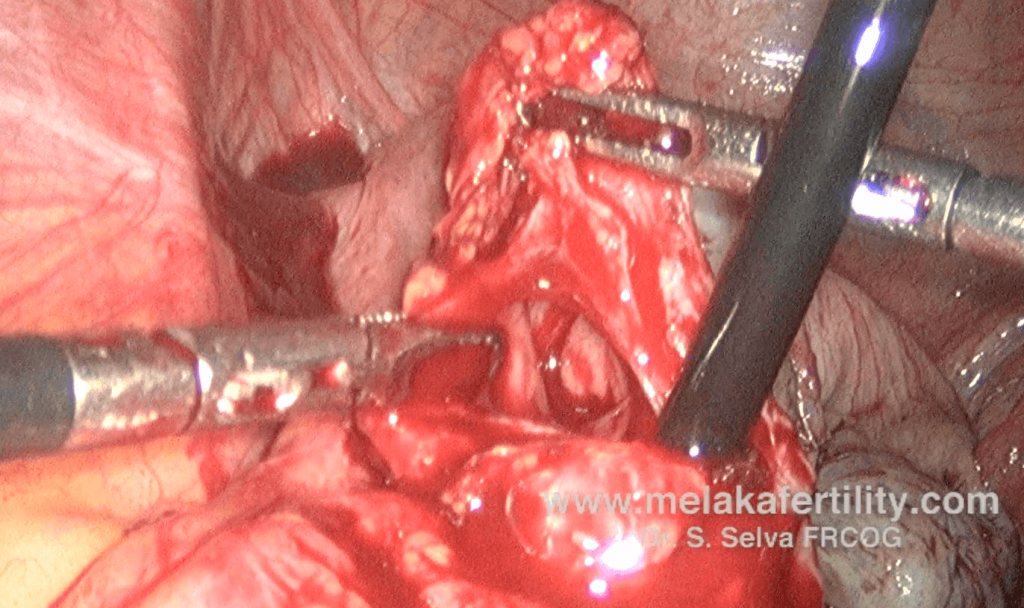
b) Placement of the secondary trocars
After placement of the first trocar (usually through the umbilicus), other trocars need to be placed. Two trocars are usually placed on either side of the abdomen. While placing these trocars, arteries (such as the inferior epigastric artery and superficial epigastric artery, may sometimes be injured, leading to bleeding. These can be sutured easily.
2) Complications Occurring during the Surgical Procedure
a) Injury to internal organs during surgery
There is always the possibility of injuring internal organs during the surgery. Organs that may be at risk of injury are the ureters, bladder, large intestines (rectum and sigmoid colon) and small intestines.
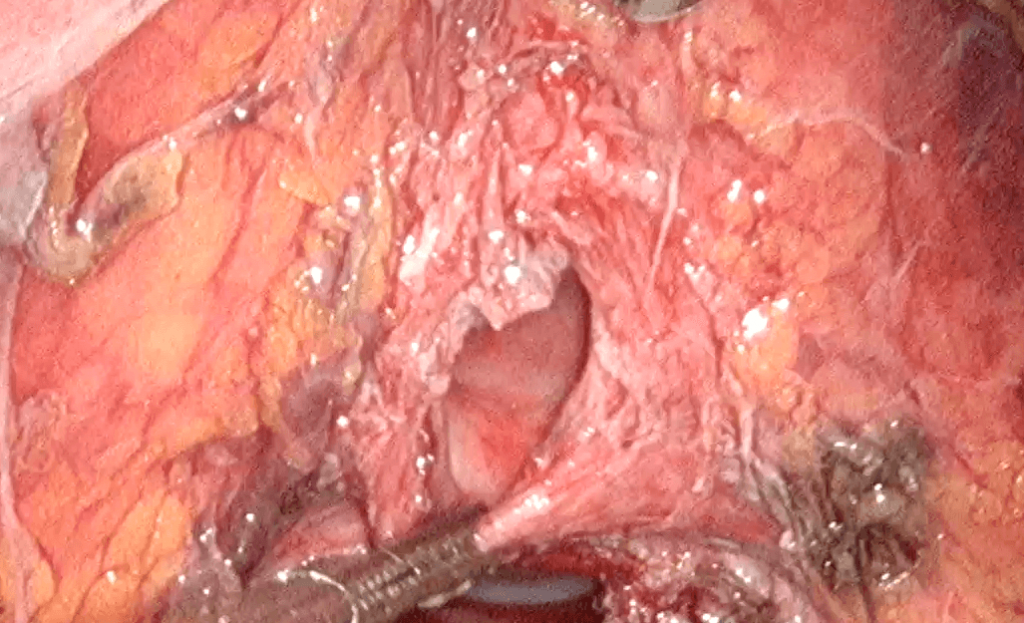
i) Ureter
The ureter is a tube that runs from the kidney to the bladder. It runs below the ovary and passes through a tunnel (ureteric tunnel) just before it reaches the bladder. Common sites of injury to the ureter are at the pelvic brim, below the ovary and at the ureteric tunnel. Certain diseases such as endometriosis sometimes causes adhesions of the ureter to the ovary and uterosacral ligament. Dissection of the ureter from the ovary/ uterosacral ligament is usually unnecessary except in difficult cases. This requires advanced laparoscopic skills. Laparoscopic surgery usually involves the use of coagulation (g) of tissues. When coagulating tissues, lateral dissipation of heat may cause accidental ureteric damage, which may not be recognised during surgery. The patient may present one week later with leakage of urine into the vagina or into the abdomen or with loin pain and fever due to stricture (narrowing) of the ureter. This complication is especially seen during laparoscopic hysterectomy, when the ascending branch of the uterine artery is coagulated and cut. Adhesions can bring the ureter closer to the uterine arteries causing accidental burns. Further surgery may be necessary to repair this injury. This may just involve placement of a plastic tube (stent) up the ureter via the bladder, so that urine will drain from the kidney to the bladder and allow healing of the injured ureter. It may sometimes be necessary to reattach the ureter into a new site in the bladder (reimplantation of the ureter). This is usually done with an open surgery.
ii) Large intestines (rectum and sigmoid)
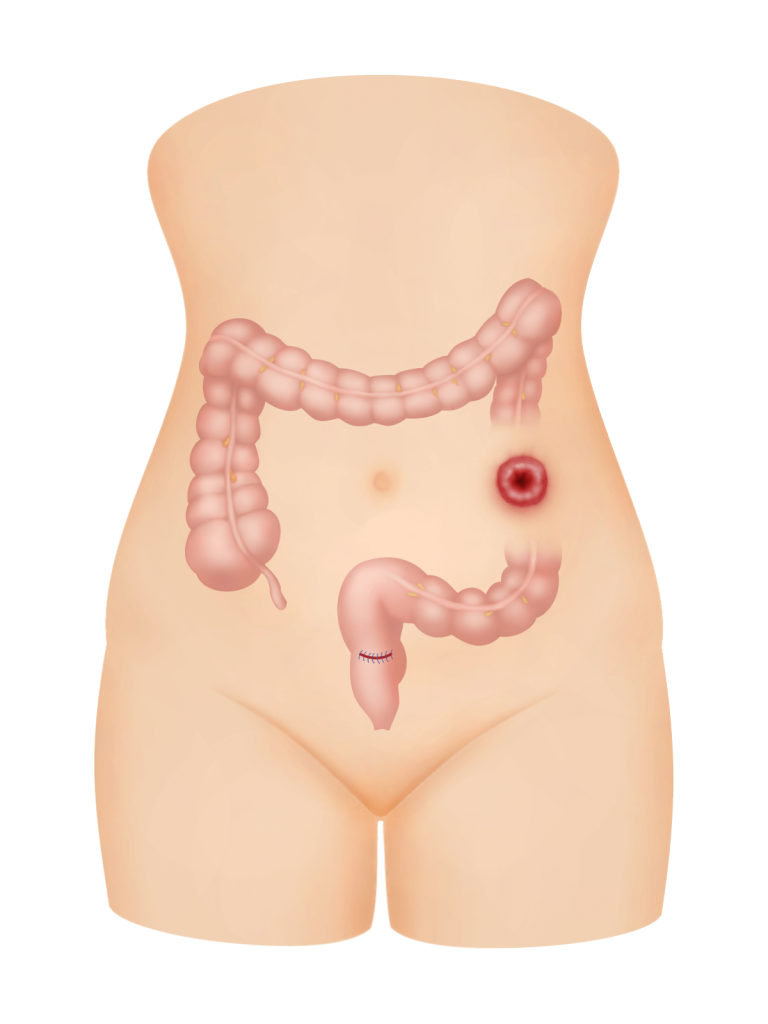
In deep infiltrating endometriosis (DIE), the disease may invade the rectum and cause dense adhesions between the rectum and the vagina, cervix and/or uterus. Releasing the bowel can lead to rectal or sigmoid colon injury. Preoperative bowel preparation is essential when such conditions are suspected. If rectal injury occurs and preoperative bowel preparation has been performed, then the injury can be repaired laparoscopically (if the surgeon is competent) or by laparotomy. However, if there is no preoperative bowel preparation, then a temporary colostomy (opening of the bowel on the abdomen) has to be done to allow healing. This is rare but can be very troublesome to the patient. Rarely is a bowel injury not suspected during surgery but manifests as a bowel leak a few days later. The patient may experience severe pelvic pain or pass out feces through the vagina. This patient may require repeat surgery either by laparoscopy or laparotomy to repair the bowel and may also need a colostomy.
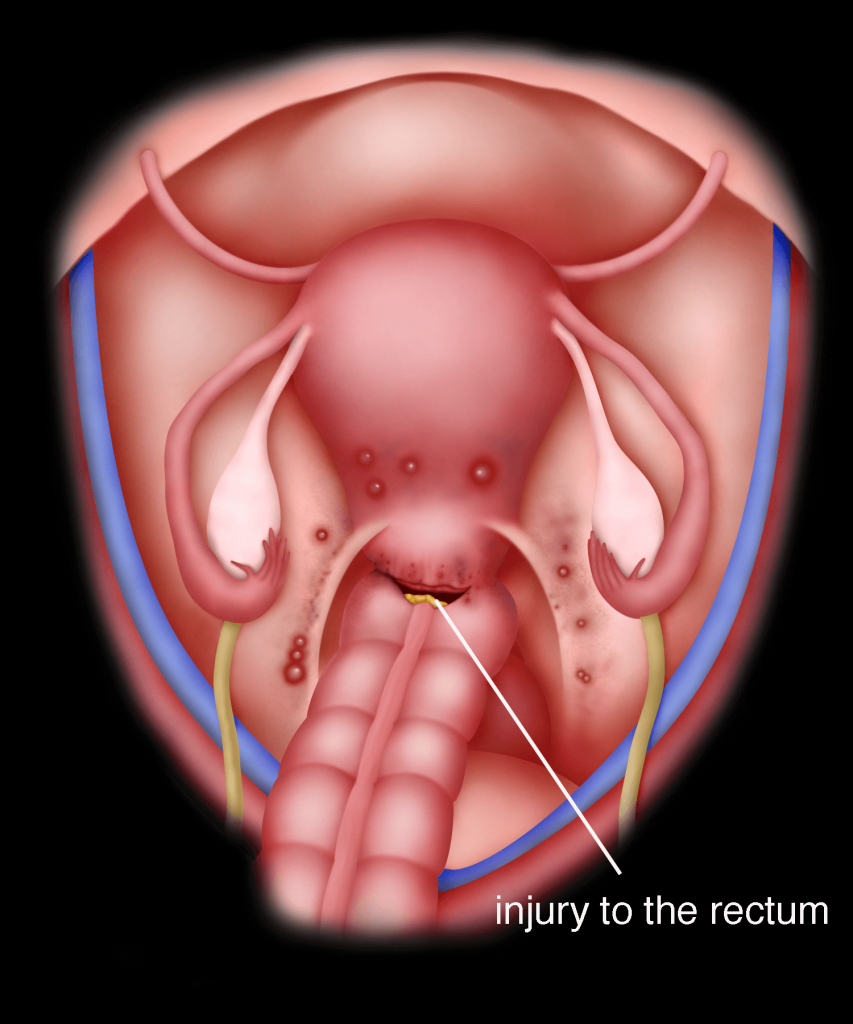
Case 17.1 : Rectal injury
A 44 year old lady consulted me in May 2007 for severe dysmenorrhoea (g) and heavy per vaginal bleeding. She had previously had a laparoscopic cystectomy. Examination revealed an enlarged uterus of 14 gestational week size (g). Nodules were felt in the Pouch of Douglas. Ultrasound showed an adenomyotic uterus with a thickened posterior wall. There was a left ovarian cyst resembling an endometioma, measuring 3.08 x 5.55 cm. She underwent a total laparoscopic hysterectomy. Upon completion of the hysterectomy, a hole was noted in the rectum. This was sutured laparoscopically using 3-0 vicryl sutures. Postoperatively, she recovered well and
was discharged well. She is still on my followup and she is well
Discussion
In patients with severe endometriosis and adenomyosis, rectal adhesion to the uterus and vagina is common. Therefore, it is necessary to do bowel preparation before the surgery, so that if bowel injury occurs, it can be repaired immediately without the need of a colostomy. It is also important in such cases to carefully release the rectum from the vagina before removing the uterus.
iii) Urinary Bladder
The urinary bladder is in front of or anterior to the uterus. It is attached loosely to the cervix. In patients who have had previous Caesarean sections, the bladder may be stuck to the cervix and uterus. In patients with large fibroids or adenomyosis, the bladder may be stretched and its position may be distorted. The bladder may also be infiltrated by endometriosis. When performing laparoscopic surgery in such situations, it may sometimes be difficult to identify the margins of the bladder so bladder injury may occur. When shaving off bladder endometriosis, a hole can be made in the bladder. If the injury is detected during surgery, the injury can easily be repaired either laparoscopically or by laparotomy. A urinary catheter has to be placed in the bladder for an extended period of time if repair of the bladder is performed. Occasionally, the injury is not detected during the surgery. The patient may present with pain and /or leakage of urine through the vagina (vesicovaginal fistula). If this occurs, than the fistula may have to be repaired either laparoscopically or by laparotomy.
Case 17.2 : Bladder injury
Madam TL, a 43 year old lady with 4 children, saw me with a complaint of pain while passing urine. Upon examination she had a 26 gestational week sized (g) uterus. Ultrasound showed a uterine fibroid measuring 9.03 x 12.09 cm. She underwent a total laparoscopic hysterectomy in August 2014. The surgery was completed without any incident. The uterus was removed by vaginal morcellation (cutting the uterus and fibroid into small pieces using a pair of scissors before removing through the vagina). The uterus and the fibroid weighed 1.32 kg. After removal of the uterus vaginally, a laparoscopy was performed and a bladder tear was seen. The bladder was repaired with vicryl 3-0 suture. Continuous suturing was performed. The vault was then sutured laparoscopically. She was discharged with a catheter on the second postoperative day. The catheter was removed on the 7th postoperative day, after a cystogram (X-ray of the bladder filled with contrast medium to make sure that the wound in the bladder has healed) showed that the bladder was intact. She is currently well.
Discussion
Injury to the bladder can occur at any stage of the surgery. In this case, it most probably occurred during vaginal morcellation of the uterus and fibroid. This is not common. My suspicion is that there was some urine in the bladder while the vaginal morcellation was performed and so the bladder was torn by the fibroid during the vaginal manipulation. It is necessary to make sure that the bladder is empty before embarking on vaginal morcellation.
iv) Small Intestines
The small intestines can be stuck to the uterus, ovaries and abdominal wall. This may be due to diseases such as endometriosis, pelvic inflammatory diseases or a result of previous operation/operations. Injury to the small intestines may occur while releasing the adhesions. Such injury, if detected during surgery can be repaired either laparoscopically or by laparotomy. As with the other organs, the injury may sometimes only be detected in the postoperative period. The patient may expe- rience abdominal distention, pain and inability to pass flatus. A second surgery may be necessary to repair the injured intestines.
Case 17.3 : Small intestine injury
Miss DI a 23 year old single lady, presented in August 2014 with the problem of slight dysmenorrhea. She had undergone a laparoscopic appendicectomy 3 year prior to seeing me. Ultrasound showed a large left endometrioma measuring 7.60 x 13.54 cm. She underwent a laparoscopy. The small bowel was densely adherent to the ovarian cyst. While releasing the small intestine, a perforation was seen. This injury was sutured with vicryl 3-0 suture using interrupted sutures. Subsequently, cystectomy was performed. Postoperatively, she was well.
Discussion
Patients with previous abdominal or pelvic surgery may have adhesions of the bowel to the female reproductive organs such as the uterus or ovary. Releasing the bowel can lead to bowel injury. It is important to warn the patient of the possible risk before surgery. Bowel injury must be diagnosed during surgery so that the patient will not have to undergo a second surgery in order to repair it.
b) Bleeding during surgery
Any form of bleeding obscures vision during laparoscopic surgery. Therefore it is vital to have as little bleeding as possible during the surgery. Bleeding from blood vessels may require a conversion to laparotomy, and blood transfusion may be necessary. However, injury to vessels can occur at any point in surgery. An example is when the Verres needle is being placed into the abdomen. This needle can injure any one of the major blood vessels such as the aorta, vena cavae or the iliac ateries or veins. When blood vessels need to be dissected out during surgery, injury may occur. This injury can be coagulated or repaired either laparoscopically or by laparotomy. On rare occasions, bleeding occurs postoperatively when a coagulated vessel opens up or a sutured vessel slips. If this occurs another surgery either by laparoscopy or laparotomy may be necessary to control the bleeding.
Case 17.4 : Postoperative bleeding
Madam JL was a 50-year-old lady. She had an abnormal cervical smear. She underwent a colposcopy and a biopsy. The biopsy confirmed that she had grade 3 cervical intraepithelial hyperplasia. She underwent a total laparoscopic hysterectomy. The surgery was uneventful and the vaginal vault was closed with no bleeding seen at the end of the surgery. She developed severe pelvic pain the next day. Pelvic ultrasound showed fluid in the Pouch of Douglas. She underwent another laparoscopy. There were 1000 mls of blood and blood clots in the pelvis. The blood and blood clots were aspirated. The left uterine artery was bleeding. The uterine artery was isolated and a clip was applied. Postoperatively, she was well.
Discussion
Laparoscopic surgery is performed with an intrabdominal pressure of between 12 and 15 mm Hg. Such pressure can mask bleeding. It is necessary to look for any evidence of bleeding with low intra abdominal pressure at the end of the surgery. Even when this is done, sometimes bleeding can occur after the surgery.
Case 17.5 : Accidental injury to the right external iliac vein during laparoscopic radical hysterectomy
Madam OLL, a 50-year-old lady, consulted me in December 2008 with irregular per vaginal bleeding. Examination revealed a cervical cancer (stage 1B). She underwent a laparoscopic radical hysterectomy and pelvic lymphadenectomy. While performing the pelvic lymphadenectomy, a small hole was accidentally made in the right external iliac vein. Fortunately, the hole did not bleed when the vein was not touched. “Surgicel®” was placed on the hole to prevent any bleeding and the surgery was continued. At the end of the surgery, no bleeding was seen from the injury. Postoperatively, there was no bleeding and the patient was discharged well.
Discussion
Accidental injury to any abdominal and pelvic organ and vessel can occur during surgery. Injury to a major vein or artery can be dangerous. In difficult cases, blood must to be cross matched and reserved in case of very heavy bleeding. Although such bleeding may be controlled by laparoscopy, laparotomy may be required.
c) Gas Embolism
The gas that is distending the abdomen can sometimes get into the blood circulation. This is called gas embolism. This rarely happens but it is a very serious complication and can be fatal. This is the reason why laparoscopic surgery is performed with the assistance of a specialist anaesthetist.
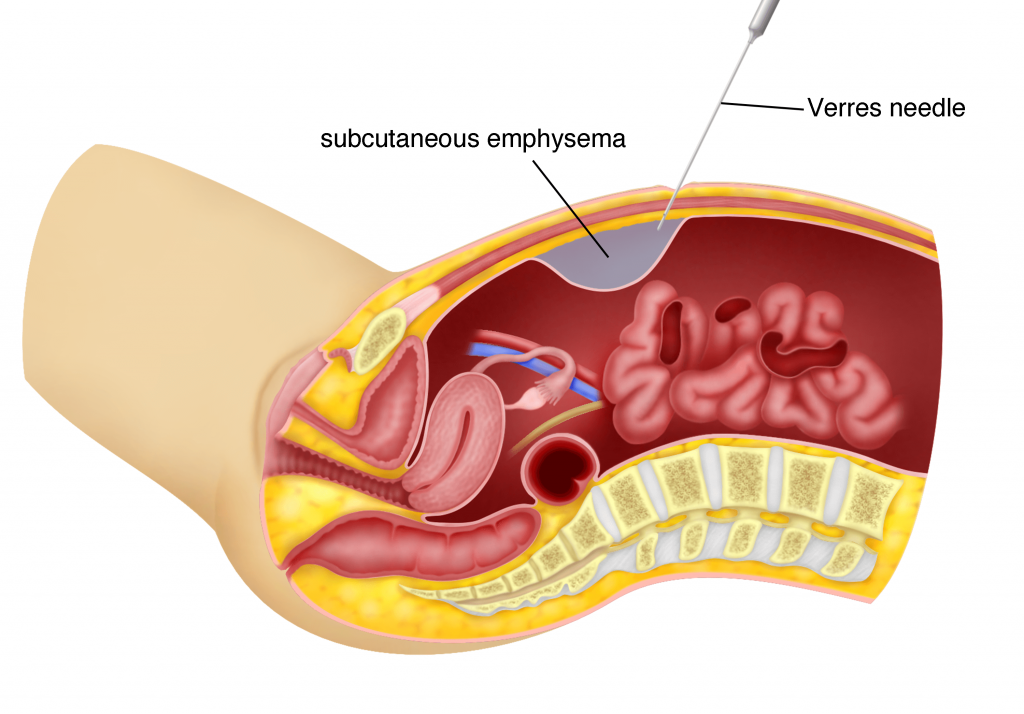
d) Subcutaneous Emphysema
Sometimes the carbon dioxide that is used to distend the abdominal cavity may leak into the subcutaneous layer (fat layer). This is called subcutaneous emphysema. This usually occurs when the Verres needle is used to insufflate the abdomen. It can even occur after trocar placement when the trocar accidentally slips into the subcutaneous layer. This is usually detected early and is not very serious. The gas is removed by reinserting the Veress needle of the trocar into the abdomen. Sometimes the emphysema is so extensive that it can go up to the neck and face. In such situations, conversion to a laparotomy may be necessary.
General Complications
1) Anaesthetic Complication
Laparoscopic surgery is performed under general anaesthesia. Difficulty in intubation, infection of the lungs and cardiac events during general anaesthesia may occur.
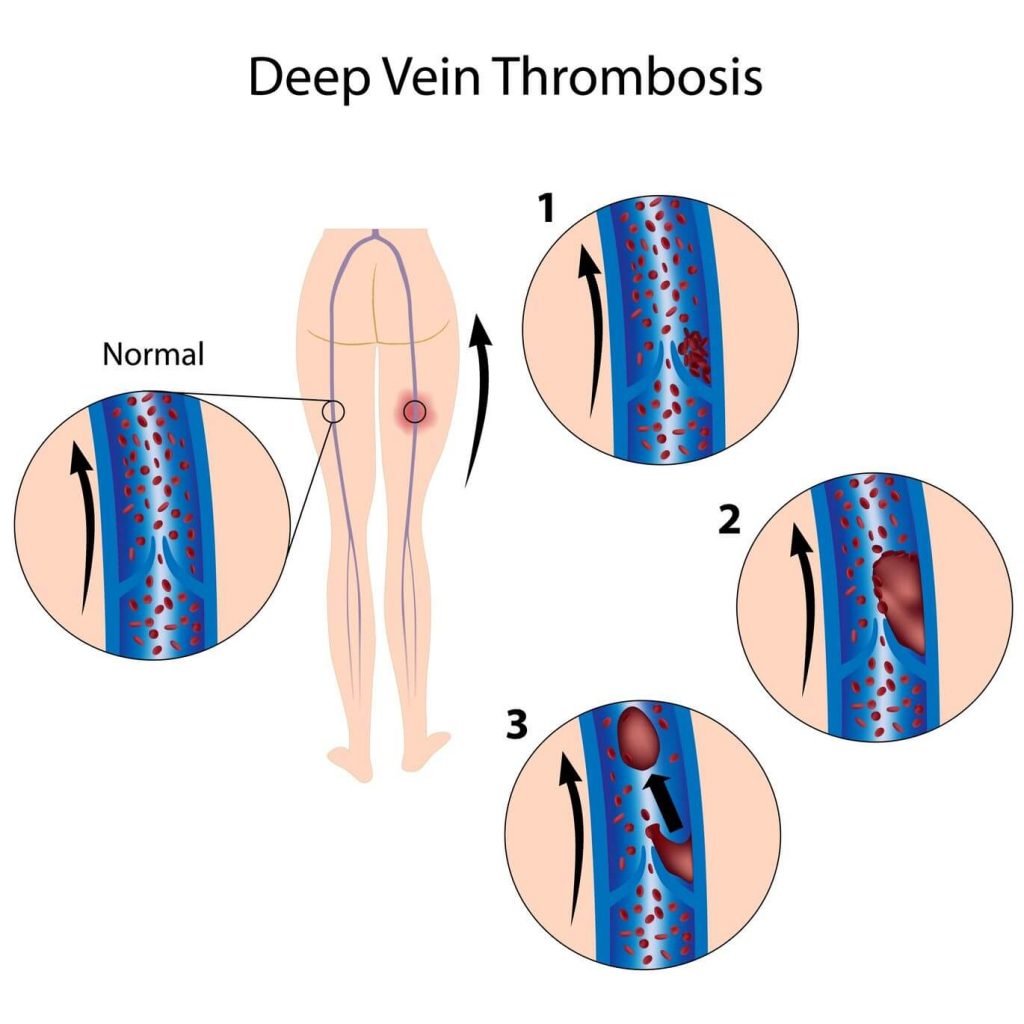
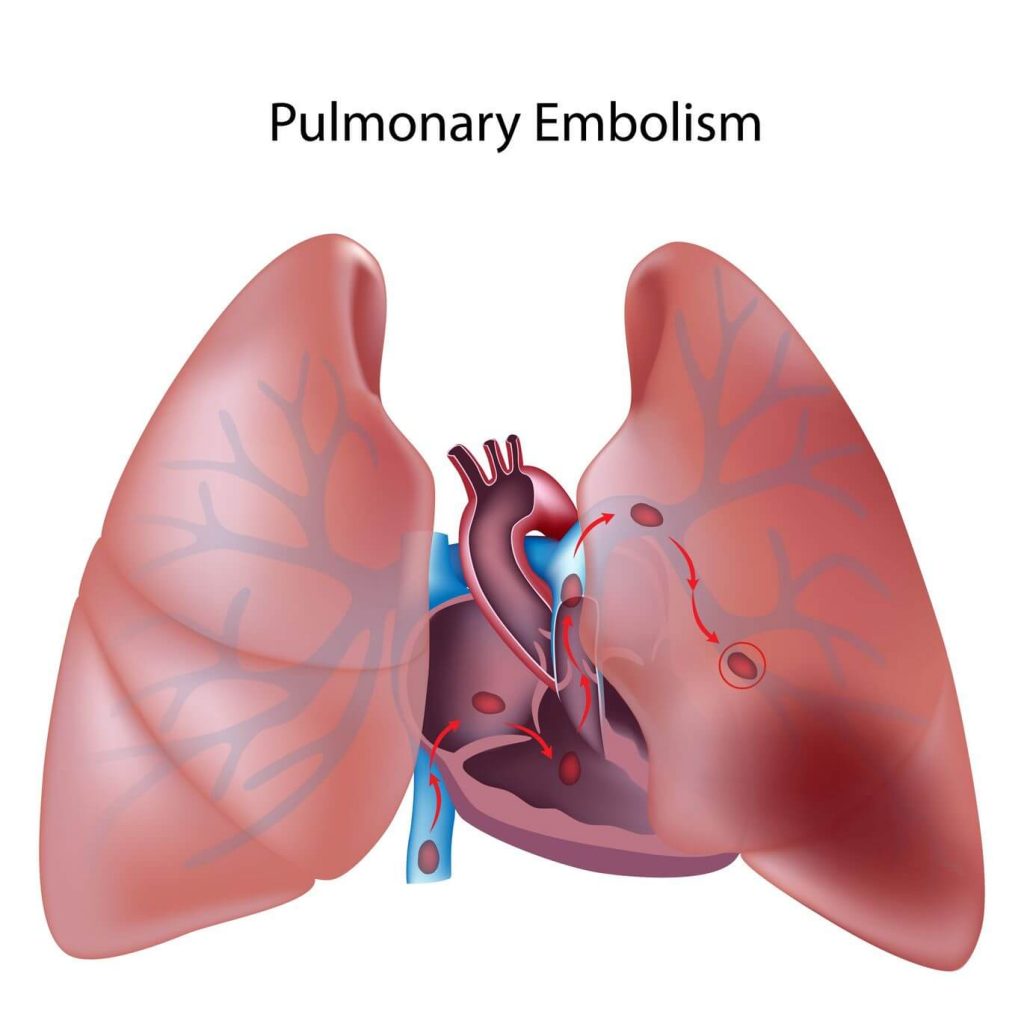
2) Deep Vein Thrombosis or Pulmonary Embolism
Blood clots may occur in the veins of the legs postoperatively. This blood clot can dislodge and move to the lungs causing pulmonary embolism. This can be life threatening. Prevention of this complication includes using stockings on the legs, using pumps and giving prophylactic heparin. The disadvantage of giving heparin prophylactically is that it may increase the incidence of intra operative and postoperative bleeding.
3) Incisional Hernia
Even though the incisions performed during laparoscopic surgery are small, sometimes abdominal contents can pass through (herniate) though them leading to incisional hernia. This may require subsequent surgery.
4) Infection
One of the advantages of laparoscopic surgery is that it is performed in a closed environment. The incidence of pelvic or abdominal infection is lower but may still occur. Laparoscopic surgery is usually performed through the umbilicus. The umbilicus is a common site for skin infection and so it is important for patients to clean the umbilicus thoroughly before coming in for surgery.

Summary
1) Complications occur in any form of surgery, may it be laparotomy or laparoscopy.
2) The more experienced a surgeon is, the less likely that a complication may occur.
3) Most complications are accidental.
4) It is important to discuss all possible complications with your doctor before embarking on a surgery.